

Iram Khatoon,1 Surrya Khanam,1 Asima Azam,2 Saima Qadeer,3 Shumaila Naz,4 Najm Ul Hassan5
1Department of Zoology, Women University Swabi, Swabi, Khyber Pakhtunkhwa, Pakistan; 2Department of Zoology, Shaheed Benazir Bhutto Women University, Peshawar, Khyber Pakhtunkhwa, Pakistan; 3Department of Zoology, Division of Science & Technology, University of Education Lahore, Lahore, Punjab, 54000, Pakistan; 4Department of Biological Sciences, National University of Medical Sciences, Rawalpindi, Punjab, Pakistan; 5Department of Microbiology, Abdul Wali Khan University, Mardan, Khyber Pakhtunkhwa, Pakistan
Correspondence: Surrya Khanam, Department of Zoology, Women University Swabi, Swabi, Khyber Pakhtunkhwa, Pakistan, Tel +923348742560, Email [email protected]
Purpose: Urinary tract infections (UTIs) are of the most common bacterial infections in Pakistan. Rapid increase in antibiotic resistance has resulted in a limited number of treatment options available. This study aimed to determine the incidence patterns of uropathogens, their antimicrobial susceptibility pattern and risk factors for UTI among the general population.
Methods: This laboratory-based cross-sectional study was conducted between November 2020 and March 2021. Urine samples were collected, cultured and bacterial isolates were identified. Bacterial isolates were tested for antimicrobial susceptibility. Data regarding socio-demographic characteristics, clinical features and risk factors were collected using structured questionnaire.
Results: Of 459 urine samples, 299 (65.1%) showed positive urine cultures (105 CFU/mL). Both gram-negative and gram-positive isolates were obtained, with a prevalence of 230 (76.9%) and 69 (23%), respectively. Escherichia coli was the predominant bacteria isolated 146 (48.8%), and it showed most susceptibility to cefoperazone and imipenem. Most of the gram-negative isolates were resistant towards ampicillin. Most risk factors were not significantly associated with UTI, except for age, income, and previous history of hospitalization.
Conclusion: UTI is an important problem in the study area, with a prevalence rate of 65%. All bacterial isolates developed resistance towards most antibiotics available on the market. Therefore, there is a need to develop management strategies based on susceptibility pattern of uropathogens. Additionally, proper public education regarding causes of disease transmission and control strategies is required.
Keywords: antimicrobial susceptibility, risks factors, urinary tract infections, Pakistan
Introduction
Urinary Tract Infection (UTI) is the occurrence of a significant number of bacteria (≥105) in the urine. UTIs are the most common bacterial infections that can be acquired from either the community or hospitals.1,2 These infections are considered an important public health concern, and approximately 150 million people per year are diagnosed with UTI, which results in economic losses of more than 6 million US dollars.3
Urinary Tract Infections (UTIs) can affect any part of the urinary system (urethra, bladder, ureters and kidney), and occur mostly in the lower urinary tract. The complications of infection also vary with the part of the urinary system involved.4 UTIs can be asymptomatic or symptomatic. Symptoms can be acute or chronic, and the severity of infection also varies from mild to severe. The clinical presentation of UTIs depends on the type of causative agent, severity of infection and immune response of the infected person.5 Although UTIs affect both sexes, females are more prone than males. Higher susceptibility in females could be due to various anatomical and physiological features such as short urethra, absence of prostatic secretion, pregnancy, and fecal contamination of the urinary tract.6 Gastrointestinal bacteria are usually involved in most UTIs, which could occur due to contamination of the rectal region and spreading of this to the urethra and bladder.7
Bacteria are considered the major causative agent of UTIs, and both gram positive and negative bacteria are involved. The major bacterial species causing UTI are Escherichia coli, Klebsiella pneumonia, Staphylococcus species, Streptococcus species, Proteus species.8 Clinical symptoms of the infections include fever, burning sensation while urinating, itching, suprapubic pain and bristle and ulcer formation in the genitals.9 Different studies have indicated several risk factors contributing to UTIs such as sex, age, past history of UTI, history of catheterization and hospitalization10 low economic status.11 The antimicrobial resistance patterns of various uropathogens vary among different countries, mainly due to the effect of antibiotic prescriptions.12,13 In some countries, due to unregulated antibiotic prescriptions, uropathogens develop serious resistance towards the drugs.14,15
Although few studies have highlighted the status of UTIs in the general population,16,17 most of the studies are restricted towards specific target groups such as HIV patients,18–20 diabetic patients,21 pregnant women,22–24 children,25,26 and students.27 Similar situation applies to our country, and limited literature on UTIs, risk factors, and drug resistance profiles are available from the general population. To develop control strategies for UTIs in the community, we need to properly diagnose pathogens, and understand the risk factors contributing to the diseases and antibiotic resistance patterns in the general population. To our knowledge, no such information is available for the present study area. A sound understanding of the various factors contributing to UTIs among the public, its prevalence rate, and the status of drug resistance in uropathogens can help healthcare planners and policymakers to develop appropriate management and control plans in the study area. Thus, the present study aimed to determine the prevalence, risk factors and antimicrobial susceptibility patterns among the general population of Swabi, Pakistan.
Methods
Study Area
This laboratory-based cross-sectional study was conducted from November 2020 to March 2021 in the Swabi District of Khyber Pakhtunkhwa, Pakistan. Urine culture, bacterial identification and susceptibility testing were conducted at the Sahara Laboratory and Diagnostic Center, Swabi.
Ethical Statement
The current study complies with the Declaration of Helsinki and ethical approval was obtained from the Ethical Committee of the Department of Zoology, Women University Swabi, Pakistan. Verbal consent was acceptable and approved by the ethical committee. The data were collected after verbal consent from all the participants. The names of the participants were not recorded, and confidentiality of the data was assured.
Study Design and Population Size
This study included adult patients with suspected UTI from different areas of Swabi district, referred to the Sahara Laboratory and Diagnostic Centre, Swabi for testing. A verbal consent was taken from all patients before data collection. A detailed questionnaire was designed to collect the data. The participants provided informed consent, and data were gathered through personal interviews. The data were collected between November 2020 and March 2021. The World Health Organization (WHO) sample size calculator was used with the following assumptions: 5% allowed error, 95% confidence interval with a statistical significance (p-value) of 0.05. The sample size was estimated to be 450, and the eligible participants were aged ≥18 years. The data collection technique was also evaluated for consistency and validity in the study population. Before the questionnaire was finalized, a pilot analysis was conducted in selected areas with 30 participants from the study area. Participants were asked to rate the phrasing, appropriateness, and clarity of the questionnaire. The structured questionnaire had high internal consistency with a Cronbach’s alpha value of 0.8. Pretest data were not included in the final analysis.
To identify the risk factors involved in the cause of urinary tract infections, and the symptoms associated with UTI, a structured questionnaire was developed following previous studies.25–28 The first section covered the socio-demographic profile of the participants including their gender, age, marital status, and monthly income. The second part consisted of a series of questions related to health, hygiene, and associated risk factors, such as history of catheterization, UTI, kidney or bladder treatment, and daily water intake. The third section was based on clinical data such as fever, dysuria, polyuria, urgency of urination, and lower back pain.
Urine Sample Collection
A sterile, wide-necked container was provided to the participants for urine sample collections. The samples were processed immediately after collection, and in case of delay in processing samples were stored in a refrigerator at 4°C.
Urine Culture and Identification of Isolates
The Bacteria were identified and cultured on Cled’s agar, MacConkey agar, Muller Hinton agar, blood agar, Mannitol Salt agar and Shigella Salmonella agar, and all the plates were incubated at 37°C for 24h. Urine sample plates were examined under a microscope to identify the appearance, morphology, color, and size of the colonies. Samples with a colony count of ≥105 cfu/mL were considered positive. Isolated bacteria were identified through colony characteristics, gram staining and different biochemical tests, namely catalase test, urease test, indole test, coagulase test, oxidase test for identification of gram-negative bacteria. Gram-positive bacteria were identified using catalase and coagulase test.23
Antibiotic Susceptibility Testing
Antibiotic susceptibility testing of bacterial isolates was performed using the Kirby-Bauer disc diffusion method according to the Clinical and Laboratory Standard Institute [CSLI] 2018 guidelines.29 A suspension of 3–5 colonies of freshly grown test organisms equivalent to 0.5 McFarland standards was prepared. The surface of the Mueller–Hinton agar was completely covered by rotating the swab with the suspension. After allowing the plates to dry for 3–5 minutes, the discs were evenly distributed on the inoculated plate with sterile forceps and incubated at 37 °C for 18–24 hours. A ruler was used to measure the diameter of inhibition zone around the discs. For each, antibiotic zones of inhibition (diameter) were measured, and bacteria were classified as susceptible, intermediate, and resistant, according to CLSI 2018 guidelines.29 The drugs used for sensitivity testing include Ampicillin (10µg), Amikacin (30μg), Amoxicillin (10µg), Amoxicillin-clavulanate (30µg), Cefixime (30µg), Cefoperazone (105µg), Ceftriaxone (30µg), Ciprofloxacin (5µg), Chloramphenicol (30µg), Ceftazidime (30µg), Cefoxitin (10µg), Clindamycin (2µg), Doxycycline (30µg), Erythromycin (5µg), Fosfomycin (50µg), Gentamicin (10µg), Imipenem (10µg), Linezolid (10µg), Levofloxacin (5µg), Nitrofurantoin (200µg), Norfloxacin (2µg), Penicillin (10µg), Trimethoprim/sulfamethoxazole (25µg), Piperacillin-tazobactam (30µg), Tigecycline (15µg), Vancomycin (10µg).
Statistical Analysis
Data were analyzed using Statistical Package for Social Science (SPSS) Version 16.0 (SPSS, Inc., Chicago, Ill). The results are presented as percentages and tables. Pearson’s Chi squared (χ2) test was used to determine the existence of association between different variables towards the occurrence of infection. Odds ratios and confidence intervals (CIs) were calculated for these parameters. All deviations with P > 0.05 were considered non-significant.
Results
Demographic Characteristics
In this study, 459 samples with UTI complaints and their associated risk factors were investigated. The majority of participants belonged to the age group 26–35 years. The mean age of the participants was 41 (±17.2 SD) with a range of 15–92 years. Of the total participants, 310 (67.5%) were female. Most of the participants were married 272 (59.3%). The majority of the participants had a monthly income between 20,000 and 40,000 PK Rupee (119–227US$) (Table 1).
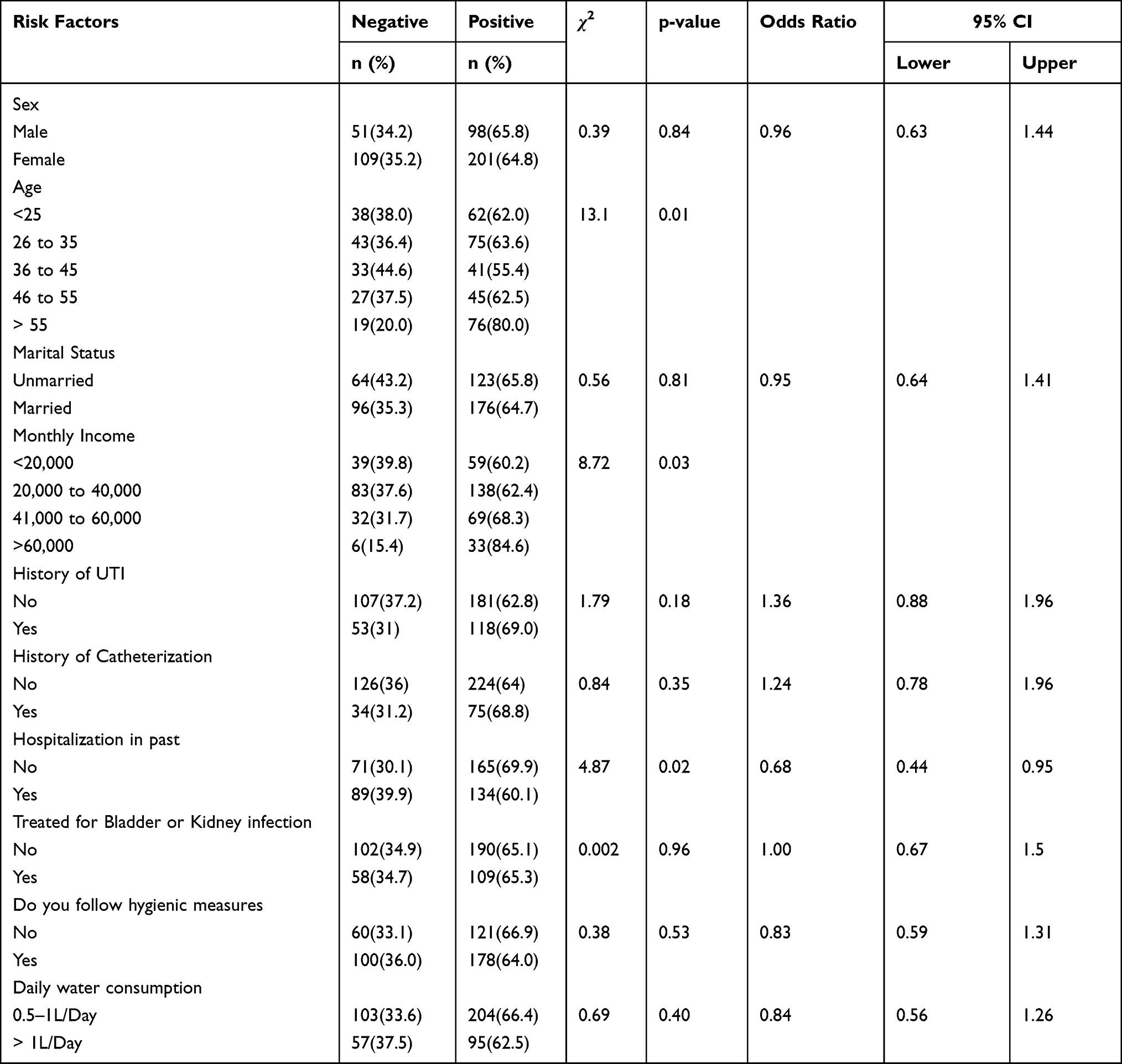 |
Table 1 Risk Factors Associated with UTI Among Population of Swabi, Pakistan (n = 459) |
Prevalence of Urinary Tract Infections
Among the 459 analyzed samples, 160 (34.8%) were negative, whereas 299 (65.1%) had positive urine culture (105 cfu/mL). The overall prevalence rate of UTI was 65.1%, and the prevalence of infections in females and males was 201 (67.2%) and 98 (32.75%), respectively. The majority of positive patients were in aged groups >55 years (25.4%) and 26–35 years (25.1%) (Table 1).
Out of 299 positive cases, 230 (76.9%) bacterial isolates were gram-negative bacteria, while 69 (23%) were gram-positive bacteria. Among the gram-negative bacterial isolates, Escherichia coli was predominant 146 (48.8%), followed by Pseudomonas aeruginosa 38 (12.70%), Klebsiella pneumoniae, 25 (8.36%) and Proteus mirabilis 21 (7%). Among the gram-positive bacteria, Staphylococcus aureus was the predominant isolate 52 (17.30%) followed by Staphylococcus saprophyticus 17 (5.68%).
Antibiotics Susceptibility Pattern of Uropathogens
Among the gram-negative bacteria, E. coli isolates were resistant to ampicillin 86.3% (n = 126), nitrofurantoin 82.2% (n = 120), and cefixime, 47.9% (n = 70). Similarly, a total of 25 Klebsiella and 38 Pseudomonas showed 100% resistant towards ampicillin. While 76% (n = 19) and 68% (n = 17), Klebsiella isolates were resistant towards Amoxicillin-clavulanate and Ceftriaxone, respectively. Among Pseudomonas isolates 78.9% (n = 30) and 63.1% (n = 24) were resistant towards amoxicillin-clavulanate and cefixime, respectively. All the 21 (100%) Proteus isolates were resistant towards ampicillin, whereas 85.7% (n = 18) were resistant towards both norfloxacin and ciprofloxacin. E. coli isolates were more susceptible to cefoperazone 58.9% (n = 86) and imipenem 52.05% (n = 76). Klebsiella pneumoniae isolates showed higher sensitivity towards imipenem 88% (n = 22) and cefoperazone 20 (80%). Pseudomonas showed full sensitivity towards cefoperazone 100% (n = 38). Proteus isolates showed complete sensitivity towards cefoxitin, imipenem, nitrofurantoin, cefoperazone and tigecycline 100% (n = 21, Table 2).
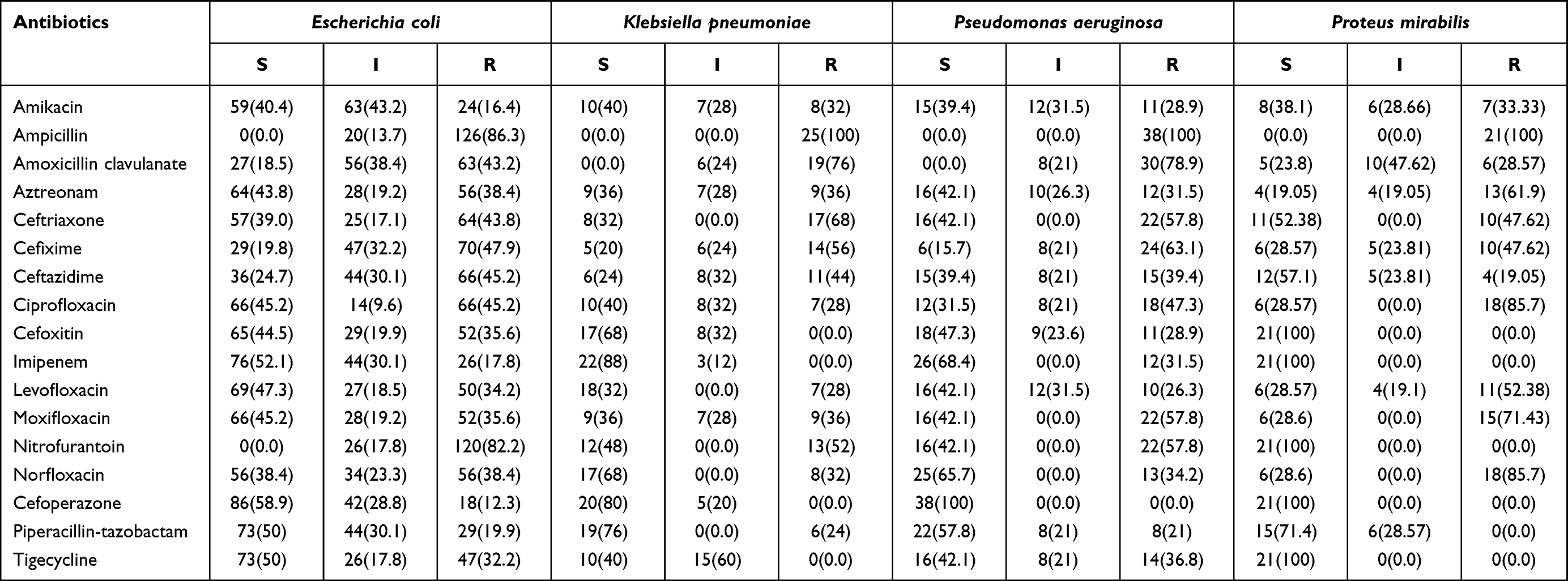 |
Table 2 Antimicrobial Susceptibility Pattern of Gram Negative Isolates Among Population of Swabi, Pakistan |
Among the gram-positive bacteria, a total of 52 Staphylococcus aureus were 100% resistant to amoxicillin, 88.4% (n = 46) to erythromycin, and 73% (n = 38) to penicillin. S. aureus isolates were sensitive towards linezolid 100% (n = 52) and vancomycin 88.4% (n = 46). Among a total of 17 Staphylococcus saprophyticus isolates 82.3% (n = 14), 70.5% (n = 12), 52.9% (n = 9) were resistant towards penicillin, cefoperazone and doxycycline, respectively. S. saprophyticus isolates were sensitive towards linezolid 100% (n = 17) and amoxicillin 94.1% (n = 16, Table 3).
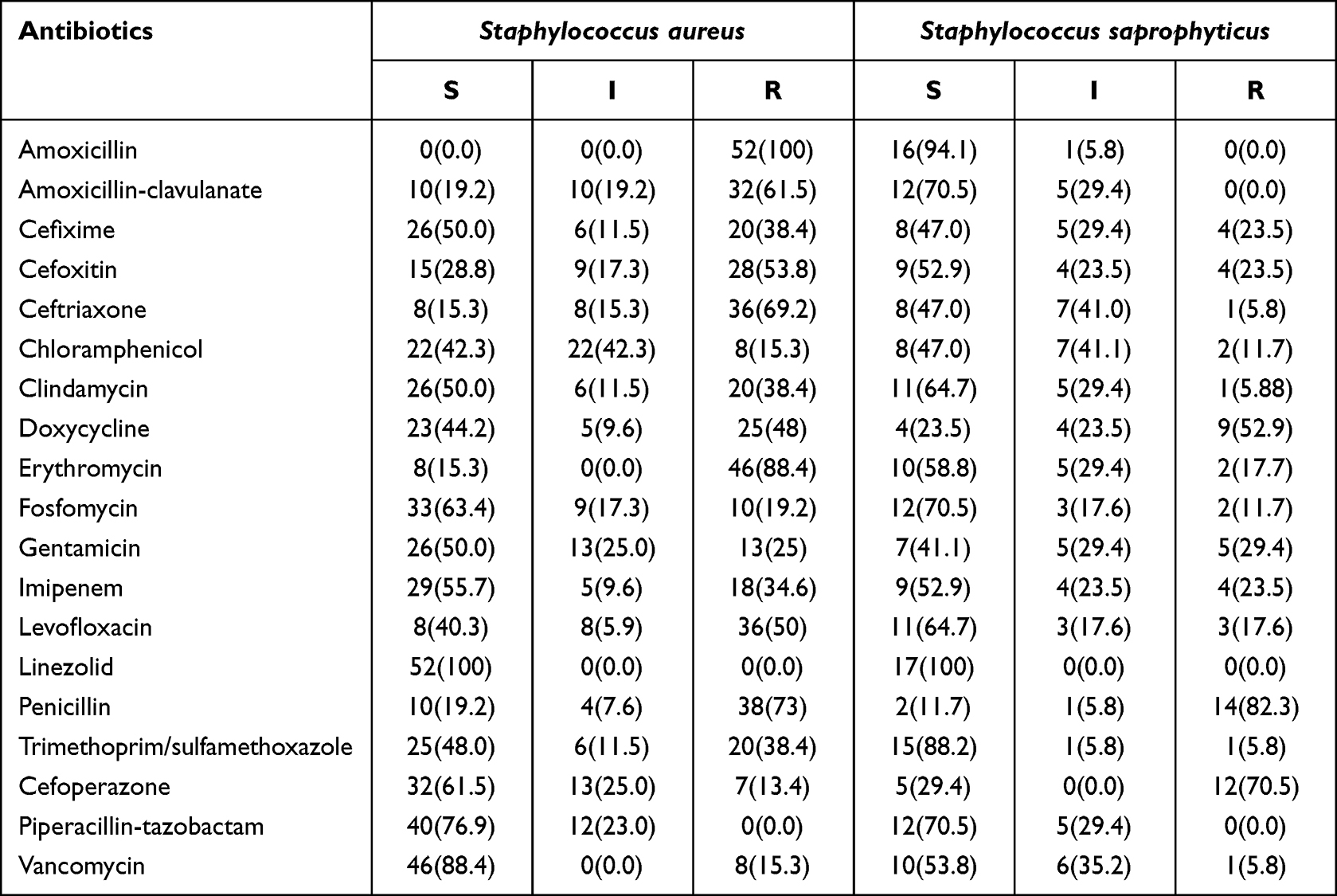 |
Table 3 Antimicrobial Susceptibility Pattern of Gram Positive Isolates Among General Population of Swabi, Pakistan |
Risk Factors and Clinical Characteristics Associated with UTI
The results showed no significant association between the different risk factors and the occurrence of UTI (P > 0.05 for all the factors), except for age (P = 0.01), monthly income (P = 0.03), and recent history of hospitalization (P = 0.02). Many of the patients were aged >55 years (n = 76) and 26 to 35 years (n = 75). In addition, most positive patients had a monthly income between 20,000 and 40,000 (Pakistani Rupee). In addition, a recent history of hospitalization was significantly associated with UTI occurrence, and the majority of positive cases were hospitalized in the recent past (Table 1).
The associations between different clinical symptoms and UTI are presented in Table 4. According to the analysis, polyuria, dysuria, hematuria, nocturia, urinary retention, lower back pain, urgency of urination, fever, itching, and hypertension were not significantly associated with the prevalence of UTI (P > 0.05), expect for diabetes mellitus (P = 0.01) which showed a negative association, and the majority of positive cases did not have the disease.
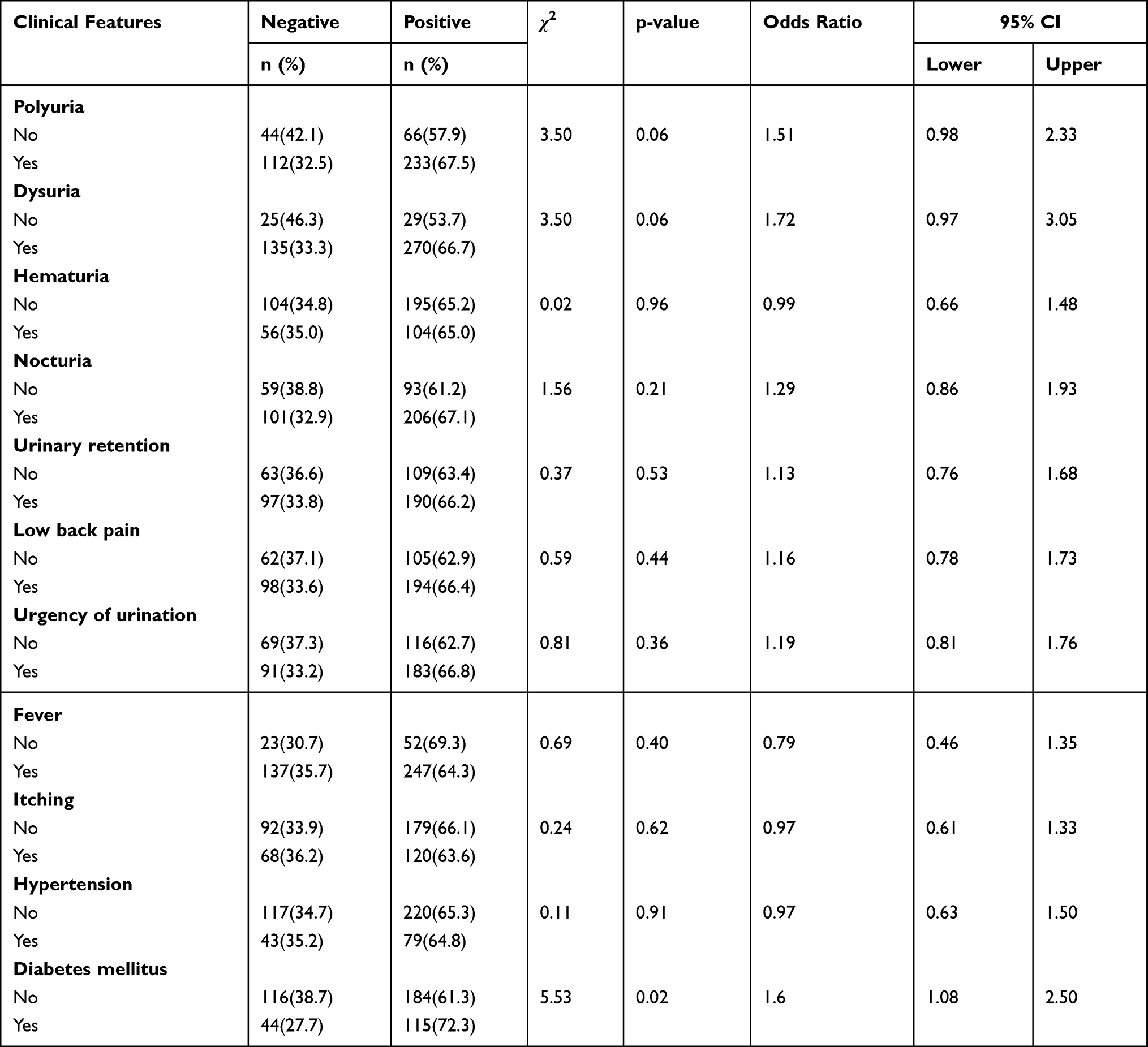 |
Table 4 Clinical Features Associated with the Occurrence of UTI Among Population of Swabi, Pakistan (n = 459) |
Discussion
The present study was conducted to assess the prevalence, causative agents, drug resistance profiles and risk factors associated with the occurrence of UTIs in the general population of Swabi, Pakistan. In this study, the prevalence of UTIs was 65.1%. The results of the present study are in agreement with those previous studies from Nigeria (60%),30 India (63.5%).31 The finding is lower than studies conducted in Bangladesh (79.5%),32 Ethiopia (90%).33 The prevalence is higher than reported in North Ethiopia (18.2%),34 South West Ethiopia (9.2%),11 Saudi Arabia (10.67%),35 Uganda (38.8%),36 and Iran (13.2%).37 Such differences could occur because of different climatic conditions, geographical variations, sanitation status or due to different levels of immune responses in the human population in different regions.
In the present study, gram-negative bacteria were the most common uropathogen found in the samples (76.9%). These results are in agreement with those of previous studies in Pakistan,38,39 Iran,40 Ethiopia11 and Canada.41 Among the gram-negative uropathogens, Escherichia coli was the predominant bacterium isolated (48.8%). Different studies from other parts of Pakistan have also reported a predominance of E. coli isolates ranging from 59% to 80%.42–45, These results are in agreement with previous studies from West Ethiopia (33.3%),11 Iran (74.6%),37 Uganda (41.9%),36 Lebanon (79.4%),46 India (48.6%)47 and Poland (73.0%).48 The reason for the predominance of Escherichia coli could be its common occurrence in anal and rectal regions. Furthermore, the predominance could be due to their unique structures, such as flagella and pili, which help to attach to the uroepithelium and therefore increase the risk of infection.48
The second most dominant gram-negative bacterium, Pseudomonas aeruginosa, in our study is consistent with work from Rawalpindi, Pakistan.38 Our study contradicted some studies where Klebsiella species, were reported as the second major isolate after Escherichia coli.,11,47,49 Among gram-positive bacteria, Staphylococcus aureus was the dominant isolate in our study, which is in agreement with previous study from Kohat, Pakistan,39 and China.50 Such difference in the type of bacterial isolates could be due to several factors such as geography, sampling methods, sampling population or hygiene practices of the population.
Antibiotics are crucial for the treatment of bacterial infections; however, their efficacy depends on the susceptibility of the etiological bacteria. Therefore, understanding the antibiotic susceptibility patterns of bacteria is important to manage all types of bacterial infections. Worldwide studies have shown that the resistance of bacteria towards antibiotics is rapidly increasing. In our study, all the gram-negative bacterial isolates showed high resistance towards ampicillin. Escherichia coli, the major isolate in the present study, showed 86.3% resistance towards ampicillin. Similarly, other three gram-negative bacteria were also completely resistant towards ampicillin (100%). This indicates that antibiotics should not be considered as antibiotic agents for UTIs. These results are in agreement with those of previous studies in Iran37 and Ethiopia.27,51 In this study, the sensitivity of gram-negative bacterial isolates towards imipenem was in agreement with that of previous study from Pakistan.16
Among the gram-positive isolates, Staphylococcus aureus showed resistance towards amoxicillin and erythromycin. This is in agreement with a previous study from Ethiopia.27 Higher sensitivity of gram-positive isolates towards Linezolid in the current study is in agreement with previous study from Pakistan.52 In our country, antibiotics are easily available at medical stores without even perceptions. Therefore, improper and inappropriate administration of antibiotics and trends in self-medication practices could be the major causes of resistance towards most antibiotics.
Our study investigated the effect of different risk factors on the prevalence of UTI. The majority of the factors were not found to be associated with the occurrence of the disease, except for age and income. In this study, prevalence was higher in the older age group (>55 years). This is in agreement with results of previous studies in India,47,53 where the prevalence was high in elderly patients. It has been reported that older males have higher UTI infection prevalence due to prostate enlargement leading to obstruction, instrumentation and neurogenic bladder.31 Similarly, older females are more affected by UTI due to the physiological and hormonal changes occurring in the body after menopause. These changes include bladder and uterine prolapse leading to incomplete bladder emptying, change in vaginal flora due to loss of estrogen, increase vaginal pH and decrease in vaginal Lactobacillus.54 In our study, the second major age group with UTI was 26–35 years. In another study, a higher prevalence was reported in the 26–40 years age group.45 This age period is considered the reproductive period, and individuals are more sexually active in these years, which may lead to UTI. With reference to income status, the UTI prevalence was high in the lower income and middle class group. This is in agreement with the results of previous studies conducted in India.47
Previous studies have reported higher prevalence of UTI among females than males.30,38,40 In our study, although females with bacteriuria outnumbered males, there was no statistically significant association between sex and the prevalence of UTI. Such variations can occur because of differences in the characteristics of the population, personal hygiene practices of the people, sampling methods, and study design.
Conclusion
In our study, the prevalence of UTI was high, and gram-negative bacteria were the most common uropathogen, with Escherichia coli as the predominant isolate. All gram-negative bacteria were highly resistant to ampicillin. The dominant isolates were sensitive towards cefoperazone and imipenem. Age and economic status were risk factors associated with UTI. Higher bacterial resistance towards most of the drugs raises concerns regarding the use of antibiotics in the area.
Acknowledgments
We are thankful to Sahara diagnostic laboratory personnel, participant for their contribution to this research work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dordevic Z, Folic M, Jankovic S. Community-acquired urinary tract infections: causative agents and their resistance to antimicrobial drugs. Vojnosanit Pregl. 2016;73:1109–1115. doi:10.2298/VSP150122218D
2. Lacovelli V, Gaziev G, Topazio L, Bove P, Vespasiani G, Finazzi Agrò E. Nosocomial urinary tract infections: a review. Urologia. 2014;81:222–227. doi:10.5301/uro.5000092
3. Foxman B. Epidemiology of urinary tract infection. Nat Rev Urol. 2010;7(12):653–660. doi:10.1038/nrurol.2010.190
4. Kucheria R, Dasgupta P, Sacks SH, Khan MS, Sheerin NS. Urinary tract infections: new insights into a common problem. Postgrad Med J. 2005;81(952):83–86. doi:10.1136/pgmj.2004.023036
5. Al-Badr A, Al-Shaikh G. Recurrent urinary tract infections management in women: a review. Sultan Qaboos Univ Med J. 2013;13:359–367. doi:10.12816/0003256
6. Olowe OA, Ojo-Johnson BB, Makanjuola OB, Olowe RA, Mabayoje VO. Detection of bacteriuria among human immunodeficiency virus seropositive individuals in Osogbo, south-western Nigeria. Eur J Microbiol Immunol. 2015;5:126–130. doi:10.1556/EuJMI-D-14-00036
7. Awaness AM, Al-Saadi MG, Aadoas SA. Antibiotics resistance in recurrent urinary tract infection. Kufa Med J. 2000;3:159.
8. John AS, Mboto CI, Agbo B. A review on the prevalence and predisposing factors responsible for urinary tract infection among adults. Eur J Exp Bio. 2016;6:7–11.
9. Mahato S, Mahato A, Yadav J. Prevalence and identification of uropathogens in Eastern Nepal and understanding their antibiogram due to multidrug resistance and ESBL. Asian Pac J Microbiol Res. 2018;2:09–17.
10. Amali O, Indinyero M, Umeh E, Awodi N. Urinary tract infections among female students of the university of agriculture, Makurdi, Benue State, Nigeria. Int J Microbiol. 2009;7:1–5.
11. Beyene G, Tsegaye W. Bacterial uropathogens in urinary tract infection and antibiotic susceptibility pattern in Jimma university specialized hospital, southwest Ethiopia. Ethiop J Health Sci. 2011;21:141–146. doi:10.4314/ejhs.v21i2.69055
12. Turpin C, Minkah B, Danso K, Frimpong E. Asymptomatic bacteriuria in pregnant women attending antenatal clinic at Komfo Anokye teaching hospital, kumasi, Ghana. Ghana Med J. 2007;41:26–29.
13. Le TP, Miller LG. Empirical therapy for uncomplicated urinary tract infections in an era of increasing antimicrobial resistance: a decision and cost analysis. Clin Infect Dis. 2001;33(5):615–621. doi:10.1086/322603
14. Goossens H, Ferech M, Vander Stichele R, Elseviers M; ESAC Project Group. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365(9459):579–587. doi:10.1016/S0140-6736(05)17907-0
15. Kanafani ZA, Mehio-Sibai A, Araj GF, Kanaan M, Kanj SS. Epidemiology and risk factors for extended-spectrum beta-lactamase-producing organisms: a case control study at a tertiary care center in Lebanon. Am J Infect Control. 2005;33:326–332. doi:10.1016/j.ajic.2005.03.009
16. Topaloglu R, Er I, Dogan BG, et al. Risk factors in community-acquired urinary tract infections caused by ESBL-producing bacteria in children. Pediatr Nephrol. 2010;25(5):919–925. doi:10.1007/s00467-009-1431-3
17. Odoki M, Almustapha Aliero A, Tibyangye J, et al. Prevalence of bacterial urinary tract infections and associated factors among patients attending hospitals in Bushenyi District, Uganda. Int J Microbiol. 2019;2019:1–8. doi:10.1155/2019/4246780
18. Tessema NN, Ali MM, Zenebe MH. Bacterial associated urinary tract infection, risk factors, and drug susceptibility profile among adult people living with HIV at Haswassa University Comprehensive Specialized Hospital, Hawassa, South Ethiopia. Sci Rep. 2020;10(1):1–9. doi:10.1038/s41598-020-67840-7
19. Ifeanyichukwu I, Emmanuel N, Chika E, et al. Frequency and antibiogram of uropathogens isolated from urine samples of HIV infected patients on antiretroviral therapy. Am J Biosci. 2013;1:50–53. doi:10.11648/j.ajbio.20130103.11
20. Marami D, Balakrishnan S, Seyoum B. Prevalence, antimicrobial susceptibility pattern of bacterial isolates, and associated factors of urinary tract infections among HIV-positive patients at Hiwot Fana specialized university hospital, Eastern Ethiopia. Can J Infect Dis Med Microbiol. 2019;2019:1–8. doi:10.1155/2019/6780354
21. He K, Hu Y, Shi JC, Zhu YQ, Mao XM. Prevalence, risk factors and microorganisms of urinary tract infections in patients with type 2 diabetes mellitus: a retrospective study in China. Ther Clin Risk Manag. 2018;14:403–408. doi:10.2147/TCRM.S147078
22. Okonko I, Ijandipe LA, Ilusanya OA, Donbraye-Emmanuel OB, Ejembi J, Udeze AO. Incidence of urinary tract infection (UTI) among pregnant women in Ibadan, South-Western Nigeria. Afr J Biotechnol. 2009;8(23):6649–6652.
23. Onuoha SC, Fatokun K. Prevalence and antimicrobial susceptibility pattern of urinary tract infection (UTI) among pregnant women in Afikpo, Ebonyi State, Nigeria. Am J Life Sci. 2014;2:46–52. doi:10.11648/j.ajls.20140202.12
24. Rahiman FO, Balasubramanian T, Shejina M, Musambil M. A review on urinary tract infection in pregnancy. Int J Pharma Res Rev. 2015;4:26–33.
25. Honkinen O, Jahnukainen T, Mertsola J, Eskola J, Ruuskanen O. Bacteremic urinary tract infection in children. Pediatr Infect Dis J. 2000;19:630–634. doi:10.1097/00006454-200007000-00009
26. Kennedy KM, Glynn LG, Dineen B. A survey of the management of urinary tract infection in children in primary care and comparison with the NICE guidelines. BMC Fam Pract. 2010;11:1–6. doi:10.1186/1471-2296-11-6
27. Gebremariam G, Legese H, Woldu Y, Araya T, Hagos K, Gebreyesus Wasihun A. Bacteriological profile, risk factors and antimicrobial susceptibility patterns of symptomatic urinary tract infection among students of Mekelle University, northern Ethiopia. BMC Infect Dis. 2019;19:1–11. doi:10.1186/s12879-019-4610-2
28. Ramzan M, Bakhsh S, Salam A, Khan GM, Mustafa G. Risk factors in urinary tract infection. Gomal J Med Sci. 2004;2:50–53.
29. Clinical and Laboratory Standards Institute. M100-Performance Standards for Antimicrobial Susceptibility Testing.
30. Kolawole AS, Kolawole OM, Kandaki-Olukemi YT, Babatunde SK, Durowade KA, Kolawole CF. Prevalence of urinary tract infections (UTI) among patients attending Dalhatu Araf Specialist Hospital, Lafia, Nasarawa state, Nigeria. Int J Med Med Sci. 2009;1:163–167. doi:10.20546/ijcmas.2018.703.060
31. Maheswary D, Saikumar C. Profile of urinary tract infections and resistance patterns in a tertiary care hospital in India. Int J Curr Microbiol Appl Sci. 2018;27(03):506–512. doi:10.20546/ijcmas.2018.703.060
32. Moue A, Aktaruzzaman SA, Ferdous N, Karim MR, Khalil MM, Das AK. Prevalence of urinary tract infection in both outpatient department and in patient department at a medical college setting of Bangladesh. Int J Biosci. 2015;7:146–152.
33. Seifu WD, Gebissa AD. Prevalence and antibiotic susceptibility of uropathogens from cases of urinary tract infections (UTI) in Shashemene referral hospital, Ethiopia. BMC Infect Dis. 2018;18(1):1–9. doi:10.1186/s12879-017-2911-x
34. Hailay A, Zereabruk K, Mebrahtom G, Aberhe W, Bahrey D. Magnitude and its associated factors of urinary tract infection among adult patients attending Tigray Region Hospitals, Northern Ethiopia, 2019. Int J Microbiol. 2020;2020:1–8. doi:10.1155/2020/8896990
35. Akbar DH. Urinary tract infection: diabetics and non-diabetic patients. Saudi Med J. 2001;22:326–329.
36. Kabugo D, Kizito S, Ashok DD, et al. Factors associated with community-acquired urinary tract infections among adults attending assessment centre, Mulago Hospital Uganda. Afr Health Sci. 2016;16:1131–1142. doi:10.4314/ahs.v16i4.31
37. Farajnia S, Alikhani MY, Ghotaslou R, Naghili B, Nakhlband A. Causative agents and antimicrobial susceptibilities of urinary tract infections in the northwest of Iran. Int J Infect Dis. 2009;13:140–144. doi:10.1016/j.ijid.2008.04.014
38. Khan IU, Mirza IA, Ikram A, et al. Antimicrobial susceptibility pattern of bacteria isolated from patients with urinary tract infection. J Coll Physicians Surg Pak. 2014;24:840–844.
39. Ullah A, Shah SRH, Almugadam BS, Sadiqui S. Prevalence of symptomatic urinary tract infections and antimicrobial susceptibility patterns of isolated uropathogens in Kohat region of Pakistan. MOJ Biol Med. 2018;3(2):85–89. doi:10.15406/mojbm.2018.03.00082
40. Angoti G, Goudarzi H, Hajizadeh M, Tabatabaii Z. Bacteria isolated from urinary tract infection among patients and determination of the antibiotic susceptibility patterns of the gram negative bacteria in Iran. Novel Biomed. 2016;4:1–4.
41. Zhanel GG, DeCorby M, Adam H, et al. Prevalence of antimicrobial-resistant pathogens in Canadian hospitals: results of the Canadian Ward Surveillance Study (CANWARD 2008). Antimicrob Agents Chemother. 2010;54(11):4684–4693. doi:10.1128/AAC.00469-10
42. Kidwai SS, Nageen A, Ghaznavi S, Bashir F, Ara J. Antibiotic susceptibility in commonly isolated pathogens from urinary tract infection in a cohort of subjects from low socioeconomic strata. Pak J Med Sci. 2017;33:254–259. doi:10.12669/pjms.332.11569
43. Amjad A, Mirza IA, Abbasi SA, Farwa U, Sattar A, Qureshi ZA. Spectrum and antimicrobial susceptibility pattern of pathogens causing urinary tract infection: experience in a tertiary care setting. Infect Dis J. 2011;20:297–301.
44. Sabir S, Anjum AA, Ijaz T, Ali MA, Khan MR, Nawaz M. Isolation and antibiotic susceptibility of E. coli from urinary tract infections in a tertiary care hospital. Pak J Med Sci. 2014;30:389.
45. Shahzad KA, Ullah F, Muhammad K, Khatoon F, Qazi MH, Ahmed I. Multiple drug resistance patterns in urinary tract infection patients in Peshawar, Khyber Pukhtunkhwa (KPK) Pakistan. J Inf Mol Biol. 2013;1:67–70.
46. Hanna-Wakim RH, Ghanem ST, El Helou MW, et al. Epidemiology and characteristics of urinary tract infections in children and adolescents. Front Cell Infect Microbiol. 2015;5:45. doi:10.3389/fcimb.2015.00045
47. Chandrasekhar D, Dollychan A, Roy BM, Cholamughath S, Parambil JC. Prevalence and antibiotic utilization pattern of uropathogens causing community-acquired urinary tract infection in Kerala, India. J Basic Clin Physiol Pharmacol. 2018;29:671–677. doi:10.1515/jbcpp-2018-0015
48. Hryniewicz K, Szczypa K, Sulikowska A, Jankowski K, Betlejewska K, Hryniewicz W. Antibiotic susceptibility of bacterial strains isolated from urinary tract infections in Poland. J Antimicrob Chemother. 2001;47:773–780. doi:10.1093/jac/47.6.773
49. Khameneh ZR, Afshar AT. Antimicrobial susceptibility pattern of urinary tract pathogens. Saudi J Kidney Dis Transpl. 2009;20:251–253.
50. Bi XC, Zhang B, Ye YK, et al. Pathogen incidence and antibiotic resistance patterns of catheter-associated urinary tract infection in children. J Chemother. 2009;21:661–665. doi:10.1179/joc.2009.21.6.661
51. Alemu A, Moges F, Shiferaw Y, et al. Bacterial profile and drug susceptibility pattern of urinary tract infection in pregnant women at university of Gondar teaching Hospital, northwest Ethiopia. BMC Res Notes. 2012;5:197. doi:10.1186/1756-0500-5-197
52. Sohail M, Khurshid M, Saleem HG, Javed H, Khan AA. Characteristics and antibiotic resistance of urinary tract pathogens isolated from Punjab, Pakistan. Jundishapur J Microbiol. 2015;8(7):e19272. doi:10.5812/jjm.19272v2
53. Eshwarappa M, Dosegowda R, Aprameya IV, Khan MW, Kumar PS. Clinico-microbiological profile of urinary tract infection in south India. Indian J Nephrol. 2011;21:30–36. doi:10.4103/0971-4065.75226
54. Kasew D, Desalegn B, Aynalem M, et al. Antimicrobial resistance trend of bacterial uropathogens at the university of Gondar comprehensive specialized hospital, northwest Ethiopia: a 10 years retrospective study. PLoS One. 2022;17(4):e0266878. doi:10.1371/journal.pone.0266878



