
Overview of the Five Point Initiative Model
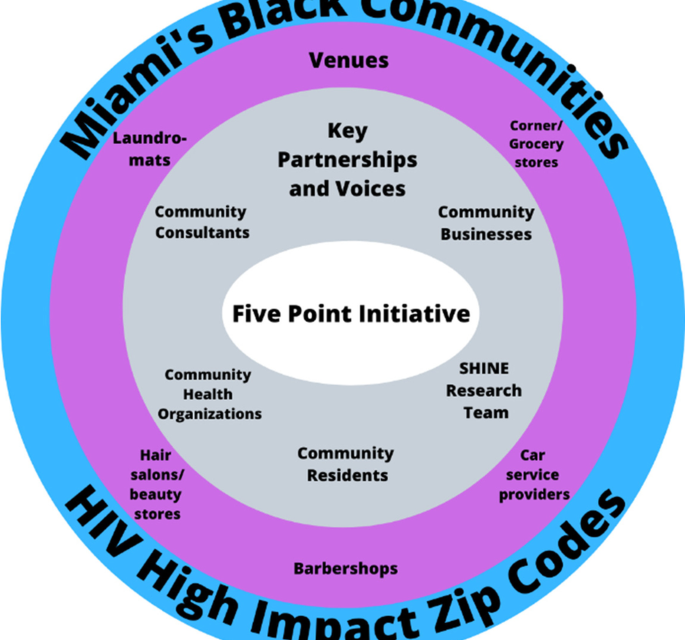
The Five Point Initiative pilot (1) partnered with five categories of businesses that Black individuals may frequent (i.e., corner/grocery stores, laundromats, salon and beauty supply stores, barbershops, and car service providers) in Miami Dade zip codes with the highest number of Black individuals living with HIV (2) closely collaborated with community health organizations funded by the Centers for Disease Control and Prevention (CDC), Health Resources and Services Administration (HRSA), and/or Substance Abuse and Mental Health Services Administration (SAMHSA) and (3) hosted outreach events in which community members complete a brief electronic survey in exchange for a service/voucher (e.g. free laundry wash and dry) at a venue with the cost being covered for by research funding and are offered HIV/STI voluntary counseling and testing on a mobile health unit, PrEP information, and condoms. Outcomes of the Five Point Initiative included (a) survey information (e.g. knowledge of and access to PrEP, barriers to care) and pilot data (acceptability and feasibility), (b) reach of Black individuals in HIV high impact zip codes in Miami who are not being reached by traditional approaches in terms of HIV prevention/treatment efforts as evidenced by lack of knowledge of PrEP and HIV testing, (c) insights from residents and business partners on our local implementation strategy, (d) condom distribution, and (e) HIV testing. As depicted (see Fig. 1), there were five key partnerships/voices and five categories of businesses with efforts targeting HIV high impact zip codes for Black individuals in Miami, FL.

Five point initiative components and context
Community consultants
Community consultants were central to the Five Point Initiative model and bring decades of expertise. One consultant had over twenty years of experience working in Black communities on HIV prevention and treatment, LGBTQ+ advocacy, harm reduction for substance use, increasing access to resources, grief counseling, and operating a faith-based ministry. The second consultant had over twenty years of experience establishing/directing nonprofits to advocate for women and girls’ sexual health and mobilizing Black women in the fight against HIV. These consultants provided key insights for planning, executing, and improving FPI, recruited businesses/venues for partnerships, and assisted with outreach events. To recruit businesses falling within the categories noted below, the consultants approached businesses (many of which they had pre-existing connections with) located in the identified HIV high impact zip codes that serve and attract Black residents and discussed FPI. Having an intimate understanding of the businesses and locations consultants also helped to inform the potential days/times for the events to maximize resident engagement.
Community businesses
Through conversations upon initial recruitment, ongoing dialogue to plan an outreach event, and exit interviews, community businesses provided insights to make the events successful and improve the approach. The five types of businesses were corner/grocery stores, laundromats, salon and beauty supply stores, barbershops, and car service providers (e.g., car wash, gas station, mechanic). Businesses distributed flyers to patrons weeks leading up to the event. The $20 vouchers provided to participants were used to purchase products or services from the businesses and generated revenue. Based on interest, neighboring businesses were simultaneously partnered with during one event.
Community health organizations
To work collectively with organizations with a shared mission to address HIV, FPI partnered with community health organizations (CHO) including clinics, local HIV prevention centers, and the department of health to provide mobile HIV testing and PrEP screening and referrals when indicated.
Residents
All community residents (18 years and older) were invited to participate during outreach events as they visited the businesses or passed nearby. Consent was obtained verbally (approved by University of Miami Institutional Review Board) and description of the research study and requirements were provided in written form and orally to participants. Residents who chose to participate completed a survey, were offered HIV testing, information on PrEP, and condoms, and received a business voucher. Residents provided satisfaction ratings, feedback, and insights as they participated and via questions at the end of the survey.
Strengthening Health through Innovation and Engagement (SHINE) research program
The research program carriers out a suite of projects (a) addressing inequities at the intersection of HIV and mental health especially among individuals minoritized due to racism (e.g., Blacks/African Americans), sexism, heterosexism, and cisgenderism and (b) engaging community members and stakeholders in research. The research team, reflective of the racial/ethnic communities most impacted by HIV, consists of the principal investigator/director, research staff, postdoctoral and doctoral students in psychology and public health, and undergraduate students. Research staff played a key role in coordinating the event logistics, all team members assisted with participant engagement at events, and oversight was provided by the principal investigator. In addition, a weekly meeting and debrief was conducted with the research team and community consultants.
HIV High-Impact Zip Codes
The piloting of FPI focused on five zip codes and Black communities in Miami, FL where HIV prevalence is high. The goal was to conduct an event at each of the five types of venues within these zip codes.
Survey administered to residents via RedCAP [38]
Residents were given the option to complete the survey on their own (using smartphone or a tablet/iPad issued by the team) or have it read by a team member. The survey was available in English, Spanish, and Haitian Creole and captured information on demographics, life experiences, mental health, substance use, physical health, sexual health, and event feedback.
Socio-demographics
Twelve questions asked about participant age, birth country, work status, household income, educational level, housing, gender identity, sex assigned at birth, relationship status, sexual orientation, racial identity, and ethnic identity.
HIV status
Participants were asked to select one of the following regarding HIV status: HIV-positive detectable viral load, HIV-positive undetectable viral load, HIV-positive I don’t know my viral load, HIV-negative, or I don’t know.
Housing stability/food insecurity
Two items were used from the United States Department of Agriculture’s 18-item scale [39] to determine food insecurity and hunger (e.g., “In the past 12 months, the food I bought just didn’t last and I didn’t have money to get more”).
Child care needs
From a national study on affordable childcare [40] we used two items (e.g., “How serious of a problem is finding quality, affordable childcare in your area?”).
Overall health
Participants were asked to rate their own health choosing from: poor, fair, good, very good, or excellent. In addition, participants were asked if they had a primary care doctor.
Mental health
From the Patient Health Questionnaire (PHQ-9) [41, 42], we used four items to assess the participant’s mood from the past two weeks (e.g. feeling down, depressed, or hopeless). In addition, participants were asked one question on self-esteem (i.e., I have high self-esteem) and one on trauma) [43].
Substance use
Two questions asked about alcohol use and drug use: “How many times in the past year have you had four or more drinks in a day?” and “How many times in the past year have you used a drug or used a prescription medication for non-medical reasons?”
Sexual health and health behaviors
Participants were asked 11 questions (varied based on HIV status and branching logic) about sexual health and health behaviors. Questions were: When was the last time you were tested for HIV? Have you ever spoken to a doctor about HIV? Have you had any sex without a condom in the past 3-months? Are you currently prescribed HIV medication?, In the last 4 weeks, how good a job did you do at taking your HIV medicine in the way you were supposed to? Have you ever heard of PrEP?, Have you ever spoken to a healthcare provider about getting PrEP?, Are you currently prescribed PrEP?, On a scale from 0-10, how important is it to you to start PrEP?, On a scale from 0-10, how confident are you that you will start using PrEP?, [30] and In the last 4 weeks, how good a job did you do at taking [PrEP] in the way you were supposed to?
Everyday discrimination
Five items were used from the Everyday Discrimination Scale [44] ( e.g., “You are treated with less courtesy or respect than other people”, “you are threatened or harassed”), which asks participants to note in their day-to-day life whether they have experienced discrimination, how frequently (e.g., almost every day, at least once a week), and to indicate the identity that was targeted (e.g., race, gender).
Barriers to medical and mental healthcare
Eight items were adapted from Heckman’s scale on barriers to care among people living with HIV [45] and assessed the following barriers for people living with and without HIV: financial reasons, HIV stigma, lack of transportation, housing, language spoken, competency of providers, shortage of mental health providers, and distance to the facilities.
Medical mistrust
Five items by LaVeist [46] on mistrust for medical facilities and personnel were used (e.g., “Hospitals have sometimes done harmful experiments on patients without their knowledge”).
Community evaluation feedback
Eight questions captured resident’s satisfaction, where residents heard about the event, activities they engaged in (e.g., testing), whether they would participate in another activity, what aspects should be in future events (e.g., voucher), and their thoughts about the event.
Exit interview with businesses
Manager/owners were asked five questions on satisfaction with the event and planning, interest in collaborating in future events, areas for improvement, and overall comments.
Statistical analyses
SPSS version 28 was used to perform all statistical analyses. All 654 participants who completed surveys were included in the quantitative analyses. Descriptive statistics (e.g., mean, standard deviation, frequencies) were computed for all quantitative variables. The brief semi-structured interviews with business partners were reviewed for common themes by two team members under the guidance of the PI.



{kind=link}