

Introduction
Primary dysmenorrhea (PD) is one of the most common gynecological conditions in women and significantly negatively impacts the quality of life.1 The increasing prevalence of PD globally has made it a public health issue.2 Despite its high prevalence, PD is often perceived as a normal part of the menstrual cycle. There is a wide variation in the prevalence of PD reported in the literature, ranging from approximately 16% to 91%, with a higher prevalence in younger women field,3–6 and 2% to 29% experienced severe pain.7
The primary pathogenesis of PD is increased production of endometrial prostaglandins.8,9 Nonsteroidal anti-inflammatory drugs are essential for treatment, and hormone therapy is available for women not planning to become pregnant.10 Many alternative therapies, such as transcutaneous electrical nerve stimulation, acupuncture, acupressure, and yoga, have been investigated.1,11,12 It is often assumed that women can self-medicate adequately, but many affected women still do not take steps to cope. Most of the previous literature summarizes a brief view of PD through cross-sectional studies, but there is significant heterogeneity between studies and a need for long-term follow-up. None of the studies comprehensively overview the hotspots and evolution in PD research themes.
Bibliometric analysis is a quantitative research method used to study and analyze patterns in scientific literature. Key components of bibliometric analysis include citation analysis, co-authorship analysis, journal analysis, and keyword analysis. In the context of bibliometric analysis, visual analysis can help researchers better understand and interpret the findings from bibliometric studies. It often involves the creation of visualizations like co-authorship networks, citation maps, and keyword clouds to convey information in a more accessible and intuitive manner. Bibliometric and visual analyses are powerful tools for evaluating the impact, trends, and dynamics within the academic literature. They are particularly valuable for researchers seeking to make data-driven decisions in various fields of science and academia. These methods continue to evolve with advances in data analytics and visualization techniques. Bibliometric and visual analyses have been widely used in the scientific field.13
Our study aims to gain deeper insights into the research landscape of primary dysmenorrhea. Biclustering analysis, facilitated by gCLUTO, allows us to identify distinct research clusters and uncover hidden patterns within the literature. Social network analysis, conducted using Ucinet, helps us understand the relationships between keywords and the importance of specific concepts within the field. Furthermore, the application of SciMAT software enables us to track the thematic evolution of research topics over time. Together, these analytical approaches provide a comprehensive understanding of the research trends, hotspots, and the evolution of primary dysmenorrhea studies, ultimately aiding researchers in making informed decisions and advancing the field.
Materials and Methods
Search Strategy
We selected the Web of Science™ Core Collection to examine all the studies related to PD. The search strategy was as follows: TS = “dysmenorrhea” OR TS = “pain menstruation” OR TS = “menstrual pain” OR TS = “pelvic pain”. The language was not limited, and publication time was also not limited. The search was completed up to 30 April 2023. Inclusion criteria were as follows: (1) human studies; (2) articles or reviews; (3) studies on PD. Exclusion criteria were: (1) animal studies; (2) secondary dysmenorrhea or dysmenorrhea before pregnancy or other systemic diseases causing dysmenorrhea. We retrieved 24,320 publications from the Web of Science™ Core Collection database. Two reviewers independently assessed each piece of literature concerning the inclusion and exclusion criteria. In case of inconsistency, a third reviewer was involved in judging until an agreement was reached. The agreement rate was 0.9 between the two independent reviewers, representing a relatively unified opinion.
Data Extraction and Bibliographic Matrix Construction
We used the Bibliographic Item Co-Occurrence Matrix Builder (BICOMB; version 2.0) software developed by Professor Lei Cui of China Medical University and VOSviewer visual analysis to extract information related to journals, countries, keywords, and citations.14 Data cleaning was completed before the keyword statistical analysis, including the unification of keywords in singular and plural, revision of misspellings, unification of full names and abbreviations, merging of keywords with close meanings, and deletion of keywords unrelated to the study content. We employed BICOMB to extract high-frequency keywords and generate a term-article matrix and a co-occurrence matrix of high-frequency keywords and highly cited literature. The term-article matrix of high-frequency keywords represents a binary structure, with high-frequency keywords forming the rows and source papers forming the columns. The number of high-frequency keywords is defined based on a threshold value.15 Finally, the high-frequency keyword occurs more than or equal to 10 times. H-index provides a reliable method for estimating a researcher’s overall scientific achievements by combining the total number of publications and citations. In essence, H-index aims to gauge the quality and quantity of scientific output cumulatively.16
Biclustering Analysis
The gCLUTO software was developed by Rasmussen at the University of Minnesota.17 This study imported a matrix of high-frequency keywords generated by BICOMB into gCLUTO version 1.0. The clustering-related parameters were set: cluster method was chosen as repeated bisection, the number of clusters was adjusted to gain the best clustering effect, similarity function was set to the correlation coefficient, criterion function was set to I2, and the other parameters were chosen as default values. A matrix visualization was employed to present the clustering results of the high-frequency keywords-source papers matrix. Additionally, a mountain map was employed to validate the clustering’s effectiveness. Based on the clustering, this study summarized the research directions of each cluster by analyzing the correlation of high-frequency keywords and the focus of illustrative papers. Finally, we identified the research hotspots of PD.
Social Network Analysis
Social network analysis is mainly used to analyze social networks’ relational structure and attributes for studying citation or collaborative relationships.18 This study used social network analysis to structure the co-high frequency keywords and co-citation network related to PD. The high-frequency keywords and highly cited papers co-occurrence matrix constructed by BICOMB was imported into Ucinet software (6.0.0.186) and NetDraw (2.0.0.84) to create a visually represented network map. The nodes represent high-frequency keywords or highly cited papers in the visual network. The position of a node depends on degree, closeness, and betweenness; the closer the node is to the center, the more central it is. The thickness of the lines connecting the nodes represents the closeness between high-frequency keywords or highly cited papers.19 Thicker lines indicate stronger connections. The distribution of nodes in the network represents the knowledge structure related to PD.
Theme Evolutionary Analysis
The software SciMAT-v1.1.04, developed by the University of Granada, was performed to analyze the development and evolution of a field. Literature was divided into three periods in this study: 1930–2009, 2010–2019, and 2020–2023, based on the characteristics of the temporal distribution of PD. The specific parameters were set as follows: words (including author and source) were selected as the unit of analysis; frequency reduction was ticked as the data reduction methods in each one time period; co-occurrence was selected as the kind of network; association strength was selected as the normalization measure; centers simples was chosen as the clustering algorithm; core mapper was selected as the document mappers; the quality measures was set H-index; Salton cosine parameters were chosen for both evolution measure and overlapping measure. The overlapping map was used to give a view of the evolution of the theme over time. The evolution map was used to study hotspots in a given period and high-frequency themes overlapping successive periods. Strategic diagrams are graphs with the X-axis denoting centrality and the Y-axis representing density. Centrality measures the external relationship between themes; density measures the internal cohesion of themes.
Results
Growth of the Literature
Overall, we retrieved and screened 903 papers through our comprehensive search process. Due to the extensive period of the papers, we listed the temporal distribution of articles by each decade (Figure 1A), which showed that the research on PD surged in the last decade. Three hundred sixty-nine journals published a study on the direction of PD from 1930 to 2023. As depicted in Figure 1B, this study revealed that the top 10 journals collectively published 276 relevant papers, representing 30.56% (276/903) of the total publications. Regarding country distribution (Figure 2), the United States had the maximum number of publications and started researching earlier. China ranked second, with Chinese researchers beginning to focus on PD in the last five years. The countries ranked 3rd to 10th were Iran, England, South Korea, Sweden, Australia, Italy, Saudi Arabia, and South Africa.
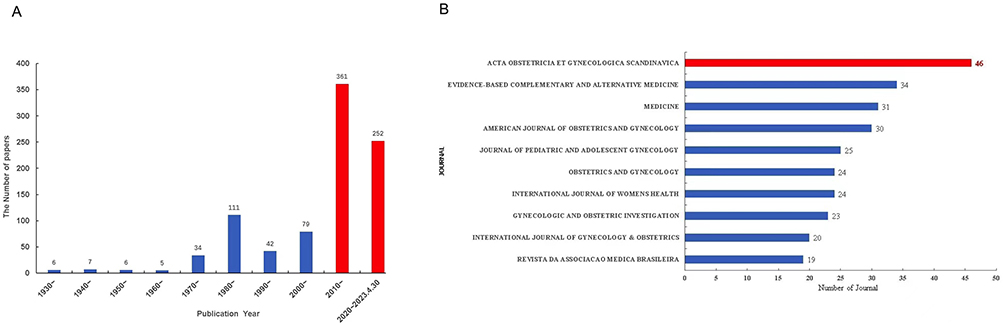 |
Figure 1 The number of articles and the published top 10 journals about primary dysmenorrhea from 1930–2023. (A) The number of articles about primary dysmenorrhea from 1930–2023 in each decade; (B) The published top 10 journals about primary dysmenorrhea from 1930–2023. |
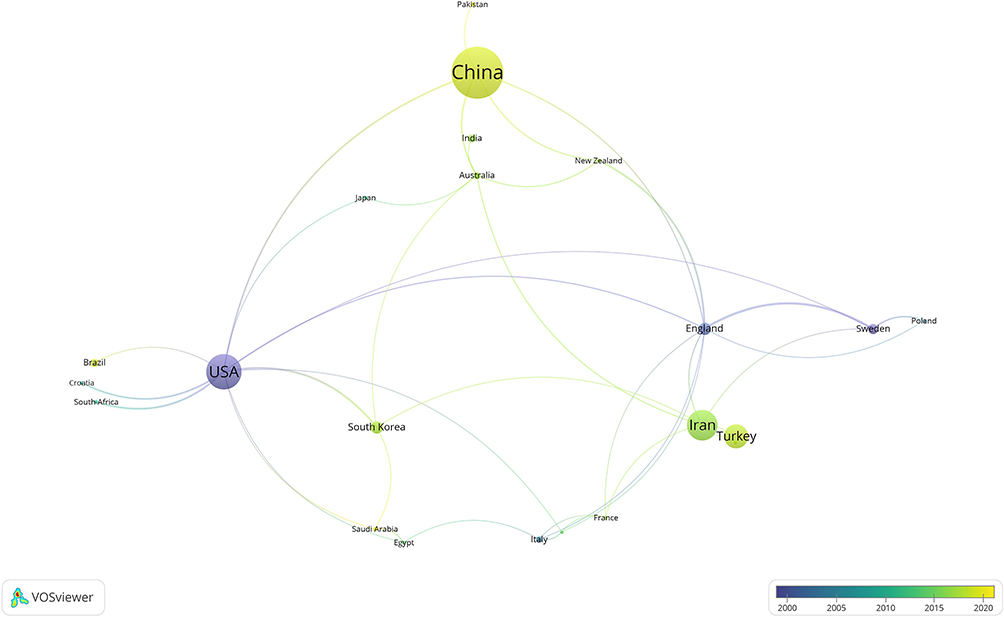 |
Figure 2 The publications on primary dysmenorrhea in the top ten most productive countries. |
Research Hotspots of PD
In this study, 44 high-frequency keywords were extracted according to the T-value calculation method, with a cumulative percentage of 46.70% (Table S1). A co-occurrence analysis was performed on the 44 high-frequency keywords to form a matrix of 44 rows*903 columns coded with “0” and “1” (Table S2). According to the actual clustering results, the 44 high-frequency keywords were finally clustered into four clusters. The results of the biclustering analysis were presented in the matrix and mountain map. The matrix visualization was presented with 44 high-frequency keywords as rows and 903 source articles as columns, with little difference in the number of high-frequency keywords within the clusters (Figure 3A). The three-dimensional visualization of the mountain (Figure 3B) provided a clear picture of the clustering of high-frequency keywords in terms of the overall layout. Mountain volume was proportional to clustered high-frequency keywords. The height was proportional to the internal resemblance of the clusters. The steeper mountains have a more remarkable internal resemblance. The color of the peak was inversely proportional to the internal standard deviation, with red representing a low standard deviation and blue representing a high standard deviation. Strongly correlated clusters may have gathering and superposition between mountains. In this study, seven research hotspots were identified based on the clustering results: epidemiological studies of PD (Cluster 0), PD causing pain hypersensitivity and central sensitization (Cluster 1), the relationship between PD and chronic pain (Cluster 1), adolescents PD (Cluster 2), PD causing changes in brain functional connectivity (Cluster 2), the current state of pharmacological treatment research (Cluster 3), the current state of non-pharmacological treatment research (Cluster 3).
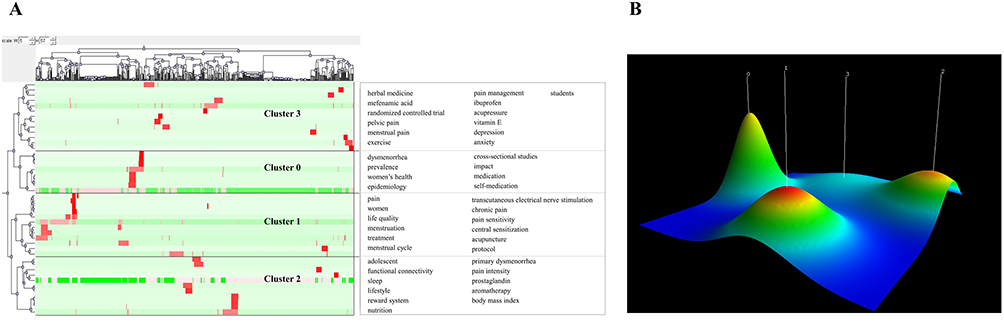 |
Figure 3 Biclustering analysis of 44 high-frequency keywords-source papers on primary dysmenorrhea. (A) Matrix visualization of biclustering of 44 high-frequency keywords and source papers on primary dysmenorrhea; (B) mountain visualization of biclustering of 44 high-frequency keywords and source papers on primary dysmenorrhea. |
Knowledge Structure of PD
The co-occurrence network of high-frequency keywords is shown in Figure 4. We evaluated node importance based on degree, betweenness, and closeness. Significant nodes were epidemiological studies on PD, PD in adolescents, pharmacological treatment, and non-pharmacological treatment. Three crucial treatment nodes were carefully selected and screened using evaluation indicators: acupuncture, acupressure, and ibuprofen. Table S3 displays the centrality of the 44 high-frequency keywords.
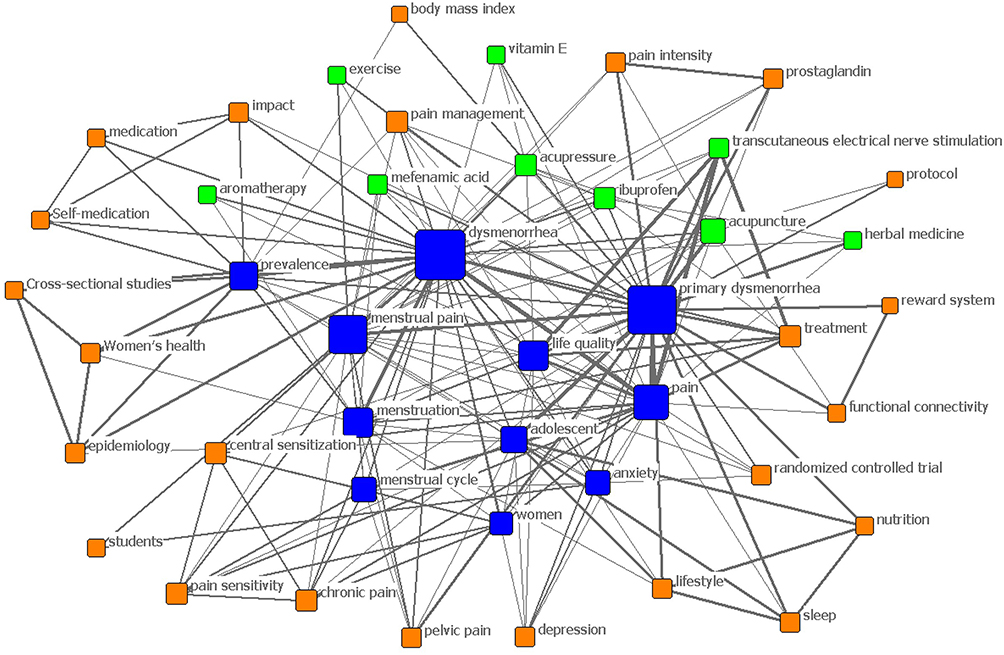 |
Figure 4 The co-occurrence network of high-frequency keywords. |
The H-index of the highly cited papers in this study was 49. According to the index value, the 48 most frequently cited papers were chosen as the highly cited papers in the reference list (Table S4). PD knowledge structure was better reflected by a co-citation network of 48 highly cited articles (Figure S1). Table S5 lists the centrality of the 48 highly cited articles. To facilitate observation of the results, the threshold of paper pairs co-occurrence was set to ≥ 40 times in this study to simplify the network of highly cited papers. Figure 5 shows Coco AS, 1999, AM FAM PHYSICIAN, V60, P489 had the highest degree of centrality, located at the network’s core. Dawood MY, 2006, OBSTET GYNECOL, V108, P428 and Iacovides S, 2015. HUM REPROD UPDATE, V21, P762 and SUNDELL G, 1990, BRIT J OBSTET GYNAEC, V97, P588 and ANDERSCH B, 1982, AM J OBSTET GYNECOL, V144, P655 had higher co-occurrence frequencies. In addition, WEI SY, 2016, PAIN, V157, P92, Tu CH, 2009, NEUROIMAGE, V47, P28 and Tu CH, 2010, PAIN, V150, P462 formed a separate structure with a focus on the structure and metabolism in the brain.
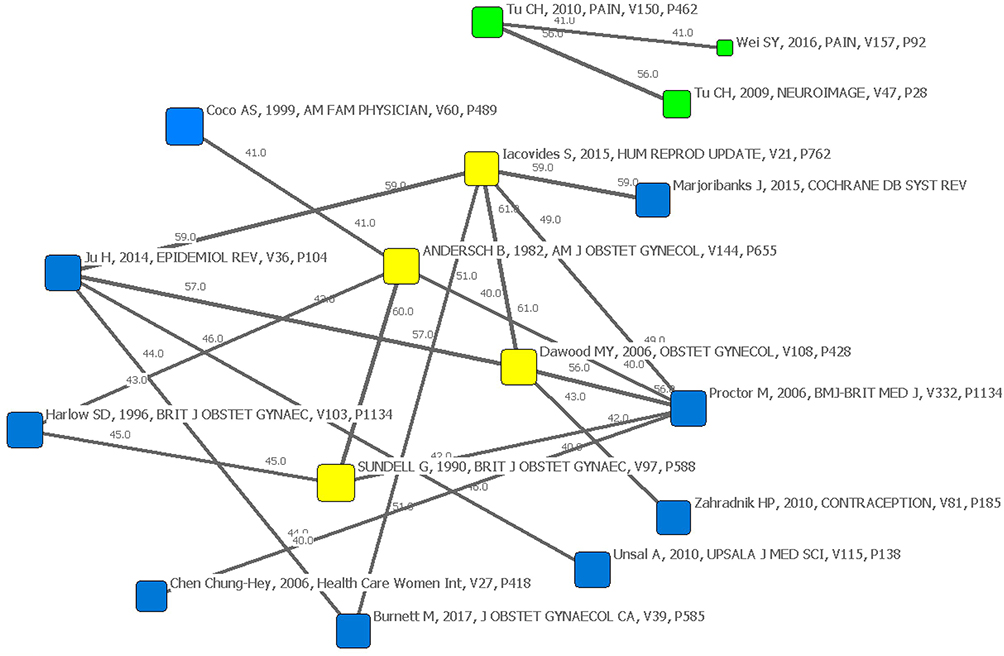 |
Figure 5 Network structure with high co-occurrence frequency of highly cited papers. |
Theme Evolution of PD
Overlapping maps illustrate the evolution of themes in PD over time. The distribution of periods is presented in Figure 6, with circles representing the themes in each period. The numbers represent the shared themes between the adjacent periods. The stability index is expressed in brackets. The higher the index, the better the stability. The arrows above the circles represent the themes change, with the inward arrow representing the number of new themes and the outward arrow representing the number of vanishing themes. The graph showed the evolution of themes in PD research, separated into three periods: 1930–2009, 2010–2019, and 2020–2023. There have been more significant new themes in the last two decades than declining ones. Notably, there has been a consistent improvement in both themes and stability index.
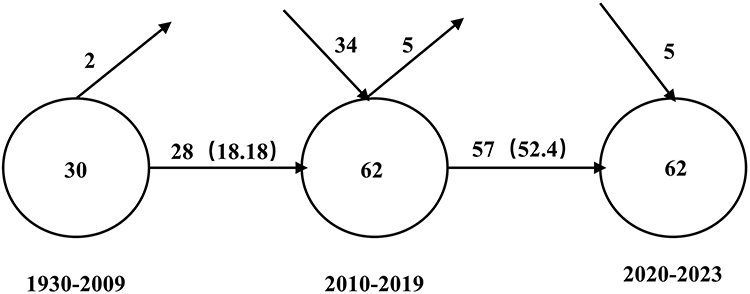 |
Figure 6 The overlapping thematic map of primary dysmenorrhea. |
Strategic diagrams represented the development status and potential of the themes. Quadrant I of Figure 7A represented a well-developed theme; quadrant II represented research that was highly developed but relatively isolated; quadrant III described research that was low in maturity and isolated (emerging or recessionary theme); quadrant IV represented research that was central but not yet mature and had great potential for development. The node’s size was proportional to the literature contained within the theme. In this study, the period of 1930–2009 (Figure 7B) was devoted to “adolescence” and “hormones”. However, 2010–2019 (Figure 7C) witnessed a shift in focus toward “receptor”. Furthermore, the more recent period of 2020–2023 (Figure 7D) exhibited a concentration of research on “fatty acids” and “clinical research”. Accordingly, the potential hotspots were “adolescence” and “randomized controlled trial”.
 |
Figure 7 Strategic diagrams for primary dysmenorrhea. (A) The interpretation of the strategic diagram; (B) strategic diagram of primary dysmenorrhea from 1930–2009; (C) strategic diagram of primary dysmenorrhea from 2010–2019; (D) strategic diagram of primary dysmenorrhea from 2020–2023. |
As demonstrated in Figure 8, the thematic evolution map was distributed vertically over three periods. The size of the nodes was proportional to the volume of literature. The thickness of the lines represented the proximity of themes. Solid lines represented the dominant direction of thematic evolution within adjacent periods, while dashed lines represented the evolution of thematic branches. Among the three periods, “adolescents” had been the focus of growing research attention. “Randomized controlled trials” appeared in third place in the 2010–2019 periods, rising to second place in the 2020–2023 periods. Moreover, pain management for PD progressed from a focus on “analgesics” in the earlier periods, transitioning to “fish oil”, and ultimately evolving into a concentration on “fatty acids” in the later periods. Notably, the circadian rhythm was found to have a limited correlation with the previous themes, indicating its emergence as a distinct and separate theme.
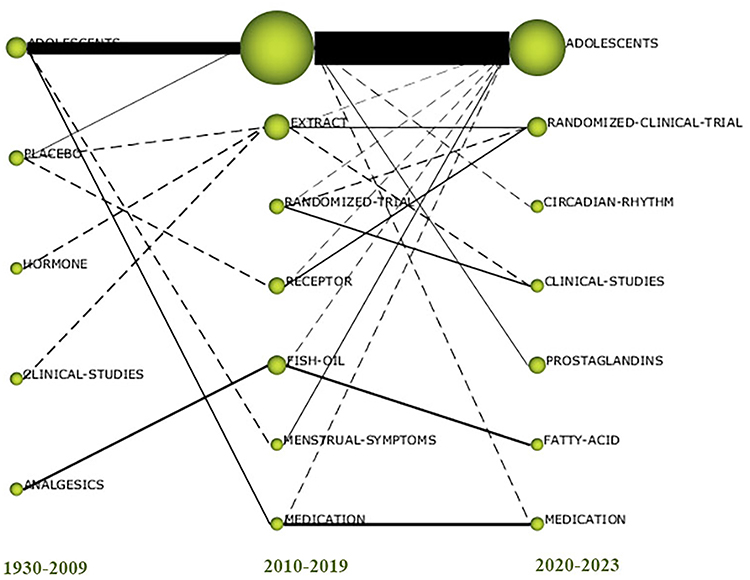 |
Figure 8 The thematic evolution map of primary dysmenorrhea. |
In essence, our work, despite drawing from known conclusions, offers a contribution by providing a systematic, organized, and accessible framework for understanding the existing literature in the field. It adds value by simplifying the research process, identifying trends, and facilitating future research endeavors.
Discussion
Our study is the first instance of utilizing bibliometric analysis to investigate the global research landscape on PD comprehensively. The number of studies conducted in developed countries could be much higher. The variations in geographical distribution can be attributed to differences in the prevalence of the condition, availability of medical and research resources, and cultural factors. Before 2009, the study on PD was in its early stages. However, from 2010 to 2019, there was a significant increase in the research volume conducted on PD. The number of published papers plateaued after 2020, when research reached a relatively mature phase. Conversely, the growth of research in adolescent PD is significantly higher than the overall level of study, which is gradually expanding and maturing.
Four themes were central to the network throughout the study period, including epidemiological studies of PD, PD in adolescents, and pharmacological and non-pharmacological treatments. These findings highlight the overarching research direction in this field, which aims to identify high-risk populations and risk factors associated with primary PD. Through epidemiological research, the goal is to explore practical strategies for preventing and treating PD.
The prevalence of PD ranges from 16% to 91%, with a higher prevalence in adolescents. Variation in most PD may be due to the lack of standard approaches for evaluating the severity of dysmenorrhea.6 Differences in study populations, medicine use, reporting systems, and symptom recall may also contribute to the variation in the diverse prevalence. Numerous cross-sectional studies conducted worldwide involving hundreds of thousands of women have revealed the following risk factors associated with PD: early age at menarche, prolonged periods, irregular periods, premenstrual symptoms, prematurity, and a family history of dysmenorrhea.20–22 Regarding psychological factors, work or life-related stress was positively associated with the risk of dysmenorrhea. Among the behavioral risk factors, smoking and alcohol consumption showed conflicting results. There was no clear association between education, marital status, physical activity, and risk of dysmenorrhea.3
Most women self-medicate using over-The-counter medication or alternative therapies, with fewer consulting a doctor. The result of the social network analysis showed three key treatment nodes, including acupuncture, acupressure, and ibuprofen. Substantial evidence supports using NSAIDs as first-line agents for treating PD.23,24 The primary mechanism is that NSAIDs could inhibit prostaglandin production and release.25 Naproxen, ibuprofen, mefenamic acid, and aspirin are all effective in PD.26 Our results showed that ibuprofen is a relatively well-studied NSAID. Oral contraceptives offer another effective treatment option, particularly for women needing birth control. It works primarily by inhibiting ovulation.27 Recently, Alternative therapies such as acupuncture, acupressure, transcutaneous electrical nerve stimulation, topical heat, and yoga have been increasingly used in recent years.28 However, there is limited and inconsistent evidence on the effectiveness of non-pharmacological treatments for PD. Social network analysis results indicate that non-pharmacological treatment studies primarily focus on acupuncture and acupressure. The meta-analysis showed that the pain severity was significantly reduced after acupuncture and acupressure.29 However, there was no difference in pain severity when the control group received sham surgery because of placebo effects.
Scientific research relies primarily on references for knowledge. The knowledge structure can be better visualized by analyzing highly cited papers from references. Epidemiological studies on PD are the most frequently co-cited. This knowledge base is, therefore, an essential background of knowledge for researchers in the field. The second knowledge base obtained from our biclustering analysis and social network analysis was the association of PD with pain hypersensitivity and chronic pain. Even though PD is prevalent, there are still significant gaps in our understanding of this condition. Evidence suggests repeated pain episodes may lead to hypersensitivity and central sensitization. The increased excitability of nociceptive projection neurons not only increases sensitivity to inputs from damaged sites but also increases sensitivity to other inputs. Prolonged injurious input to the central nervous system can induce functional and structural changes throughout the nervous system. Studies have shown structural changes in the brain of dysmenorrhea women, such as lower grey matter volumes in regions involved in pain transmission and sensory processing while a larger grey matter volume in regions involved in pain modeling and regulation of endocrine function.30,31 Further research should determine whether effective blockade of PD can improve the development of chronic pain.
Based on our thematic evolutionary analysis, we predicted that dietary supplements would be the following hotspot for PD. Our strategic diagrams showed that research on fatty acids might go back even further, which evolved from the original “analgesics” to “fish oil” and finally to “fatty acids”. Studies have shown that n-3 polyunsaturated fatty acid can improve PD in adolescents.32 The mechanism for this is that n-3 polyunsaturated fatty acid reduces prostaglandin and leukotrienes. The therapeutic effect of low doses of n-3 polyunsaturated fatty acid is optimal and decreases with increasing daily intake. Another finding showed that n-3 polyunsaturated fatty acid supplementation was less effective in reducing the severity of PD as women aged.33 Vitamin E may also relieve PD by inhibiting the activity of phospholipase A2 and cyclooxygenase.34,35 Dietary supplements are widely popular among women and readily available in pharmacies and supermarkets. Furthermore, more high-quality evidence for dietary supplements for PD needs to be provided. Randomized controlled trials should consider dose, quality, and drug interactions.
Our biclustering and thematic evolutionary analysis suggested that adolescent PD had always been a research hotspot in this field. The main reason might be the high prevalence of PD in adolescents and its high co-morbidity with many functional pain disorders. In recent years, there has been a focus on functional connectivity, which is the functional interaction between different brain areas. Studies have shown that the functional connectivity of the periaqueductal grey matter plays a significant role in the neural axis of the regulatory system of PD.36 The low correlation between the periaqueductal grey and the default mode network is a common endpoint in many functional pain disorders (migraine, fibromyalgia, and temporomandibular joint disorder). The findings suggested that women with long-term PD may develop adaptive neuroplasticity and functional reorganization, shifting the network from salient emotional processing to cognitive pain regulation. Preventing the development of PD in adolescence and actively treating moderate to severe PD may have clinical implications for preventing chronic pain. Our research highlights the importance of further investigation to comprehend this disorder and its long-term consequences. It is noteworthy that lifestyle changes can improve the quality of life and decrease pain levels in individuals with primary dysmenorrhea.37 We urge researchers to explore genetic predispositions, lifestyle factors, and early interventions impact on long-term outcomes.
Based on our thematic evolutionary analysis, the circadian rhythm was not closely related to the previous themes. It emerged independently in the third period, suggesting it may be an emerging theme. Based on our analysis, we anticipate that sleep disorders associated with PD hold promising academic potential. Additionally, the study found that the variable number of Tandem repeat variants in the Coding Region of the Circadian rhythm gene cycle 3 affects sleep, which may also be associated with PD in Turkish women.38 However, further studies in ethnically diverse populations are needed to address the full role of this variant in PD.
This study does have certain limitations that should be acknowledged. Firstly, we only collected data from a single Web of Science™ Core Collection database. Secondly, we only included articles and reviews from human studies, which may miss other research hotspots. In addition, biclustering analysis and social network analysis based on high-frequency keywords may lead to some emerging topics being overlooked.
Conclusion
In conclusion, our study identified seven research hotspots, three key treatment nodes, and four research trends related to PD. These findings enhance our understanding of the knowledge structure associated with PD. Our study contributes to the scientific understanding of PD and its broader implications for women’s health, inspiring innovative approaches to address the challenges posed by this condition. Through continued research efforts, we can improve the quality of life for affected women and transform PD management.
Abbreviation
PD, primary dysmenorrhea.
Data Sharing Statement
The datasets used and analyzed during the course of this study are available from the corresponding author upon reasonable request.
Acknowledgments
Thanks to the Library of China Medical University for providing electronic data resources and to all the peer reviewers for their opinions and suggestions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferries-Rowe E, Corey E, Archer JS. Primary dysmenorrhea: diagnosis and therapy. Obstet Gynecol. 2020;136(5):1047–1058. doi:10.1097/AOG.0000000000004096
2. Liu Z, Li Z, Meng Q, Gu Z, Cui J. Bibliometric analysis of global research landscape and hotspots on dysmenorrhea: where are we now? J Pain Res. 2023;16:269–285. doi:10.2147/JPR.S396083
3. Ju H, Jones M, Mishra G. The prevalence and risk factors of dysmenorrhea. Epidemiol Rev. 2014;36:104–113. doi:10.1093/epirev/mxt009
4. Iacovides S, Avidon I, Baker FC. What we know about primary dysmenorrhea today: a critical review. Hum Reprod Update. 2015;21(6):762–778. doi:10.1093/humupd/dmv039
5. Bernardi M, Lazzeri L, Perelli F, Reis FM, Petraglia F. Dysmenorrhea and related disorders. F1000Research. 2017;6:1645. doi:10.12688/f1000research.11682.1
6. Karout S, Soubra L, Rahme D, Karout L, Khojah HMJ, Itani R. Prevalence, risk factors, and management practices of primary dysmenorrhea among young females. BMC Womens Health. 2021;21(1):392. doi:10.1186/s12905-021-01532-w
7. De Sanctis V, Soliman A, Bernasconi S, et al. Primary dysmenorrhea in adolescents: prevalence, impact and recent knowledge. Pediatr Endocrinol Rev. 2015;13(2):512–520.
8. Itani R, Soubra L, Karout S, Rahme D, Karout L, Khojah HMJ. Primary dysmenorrhea: pathophysiology, diagnosis, and treatment updates. Korean J Fam Med. 2022;43(2):101–108. doi:10.4082/kjfm.21.0103
9. Guimarães I, Póvoa AM. Primary dysmenorrhea: assessment and treatment. Rev Brasileira de Ginecol Obstet. 2020;42(8):501–507. doi:10.1055/s-0040-1712131
10. Harel Z. Dysmenorrhea in adolescents and young adults: an update on pharmacological treatments and management strategies. Expert Opin Pharmacother. 2012;13(15):2157–2170. doi:10.1517/14656566.2012.725045
11. Kanchibhotla D, Subramanian S, Singh D. Management of dysmenorrhea through yoga: a narrative review. Front Pain Res. 2023;4:1107669. doi:10.3389/fpain.2023.1107669
12. Cao M, Ye F, Xie W, Yan X, Ho MH. Effectiveness of auricular acupoint therapy targeting menstrual pain for primary dysmenorrhea: a systematic review and meta-analysis of randomized controlled trials. Worldviews Eviden Bas Nurs. 2023;29. doi:10.1111/wvn.12636
13. Chen C, Dubin R, Kim MC. Emerging trends and new developments in regenerative medicine: a scientometric update (2000 – 2014). Expert Opin Biol Ther. 2014;14(9):1295–1317. doi:10.1517/14712598.2014.920813
14. Li F, Li M. Mapping publication trends and identifying hot spots of research on Internet health information seeking behavior: a quantitative and co-word biclustering analysis. J Med Internet Res. 2015;17(3):e81. doi:10.2196/jmir.3326
15. Donohue JC. Understanding Scientific literatures—A Bibliometric Approach. Cambridge: MIT Press; 1974:49–50.
16. Hirsch JE. An index to quantify an individual’s scientific research output. Proc Natl Acad Sci USA. 2005;102(46):16569–16572. doi:10.1073/pnas.0507655102
17. Rasmussen M, Karypis G. gCLUTO – an interactive clustering, visualization, and analysis system. UMN Technical Report; 2004.
18. Pandia MK, Bihari A. Important author analysis in research professionals’ relationship network based on social network analysis metrics; 2015.
19. Gu D, Li J, Li X, Liang C. Visualizing the knowledge structure and evolution of big data research in healthcare informatics. Int J Med Inform. 2017;98:22–32. doi:10.1016/j.ijmedinf.2016.11.006
20. Hu Z, Tang L, Chen L, Kaminga AC, Xu H. Prevalence and risk factors associated with primary dysmenorrhea among Chinese female university students: a cross-sectional study. J Pediatr Adolesc Gynecol. 2020;33(1):15–22. doi:10.1016/j.jpag.2019.09.004
21. Al-Husban N, Odeh O, Dabit T, Masadeh A. The influence of lifestyle variables on primary dysmenorrhea: a cross-sectional study. Inter J Women’s Health. 2022;14:545–553. doi:10.2147/ijwh.s338651
22. Wang L, Yan Y, Qiu H, et al. Prevalence and risk factors of primary dysmenorrhea in students: a meta-analysis. Value Health. 2022;25(10):1678–1684. doi:10.1016/j.jval.2022.03.023
23. Dawood MY. Nonsteroidal anti-inflammatory drugs and changing attitudes toward dysmenorrhea. Am J Med. 1988;84(5A):23–29. doi:10.1016/0002-9343(88)90473-1
24. Kaplan Ö, Nazıroğlu M, Güney M, Aykur M. Non-steroidal anti-inflammatory drug modulates oxidative stress and calcium ion levels in the neutrophils of patients with primary dysmenorrhea. J Reprod Immunol. 2013;100(2):87–92. doi:10.1016/j.jri.2013.10.004
25. Whelton A. Nephrotoxicity of nonsteroidal anti-inflammatory drugs: physiologic foundations and clinical implications. Am J Med. 1999;106(5B):13S–24S. doi:10.1016/s0002-9343(99)00113-8
26. Zhang WY, Li Wan Po A. Efficacy of minor analgesics in primary dysmenorrhoea: a systematic review. Br J Obstet Gynaecol. 1998;105(7):780–789. doi:10.1111/j.1471-0528.1998.tb10210.x
27. Kho KA, Shields JK. Diagnosis and management of primary dysmenorrhea. JAMA. 2020;323(3):268–269. doi:10.1001/jama.2019.16921
28. Kannan P, Claydon LS. Some physiotherapy treatments may relieve menstrual pain in women with primary dysmenorrhea: a systematic review. J Physiother. 2014;60(1):13–21. doi:10.1016/j.jphys.2013.12.003
29. Abaraogu UO, Tabansi-Ochuogu CS. As acupressure decreases pain, acupuncture may improve some aspects of quality of life for women with primary dysmenorrhea: a systematic review with meta-analysis. J Acupunct Meridian Stud. 2015;8(5):220–228. doi:10.1016/j.jams.2015.06.010
30. Tu CH, Niddam DM, Chao HT, et al. Brain morphological changes associated with cyclic menstrual pain. Pain. 2010;150(3):462–468. doi:10.1016/j.pain.2010.05.026
31. Tu CH, Niddam DM, Yeh TC, et al. Menstrual pain is associated with rapid structural alterations in the brain. Pain. 2013;154(9):1718–1724. doi:10.1016/j.pain.2013.05.022
32. Rahbar N, Asgharzadeh N, Ghorbani R. Effect of omega-3 fatty acids on intensity of primary dysmenorrhea. Int J Gynaecol Obstet. 2012;117(1):45–47. doi:10.1016/j.ijgo.2011.11.019
33. Mohammadi MM, Mirjalili R, Faraji A. The impact of omega-3 polyunsaturated fatty acids on primary dysmenorrhea: a systematic review and meta-analysis of randomized controlled trials. Eur J Clin Pharmacol. 2022;78(5):721–731. doi:10.1007/s00228-021-03263-1
34. Ziaei S, Zakeri M, Kazemnejad A. A randomised controlled trial of vitamin E in the treatment of primary dysmenorrhoea. BJOG. 2005;112(4):466–469. doi:10.1111/j.1471-0528.2004.00495.x
35. Matsas A, Sachinidis A, Lamprinou M, Stamoula E, Christopoulos P. Vitamin effects in primary dysmenorrhea. Life. 2023;13(6):1308. doi:10.3390/life13061308
36. Wei SY, Chao HT, Tu CH, et al. Changes in functional connectivity of pain modulatory systems in women with primary dysmenorrhea. Pain. 2016;157(1):92–102. doi:10.1097/j.pain.0000000000000340
37. Dogan H, Eroglu S, Akbayrak T. The effect of kinesio taping and lifestyle changes on pain, body awareness and quality of life in primary dysmenorrhea. Complement Ther Clin Pract. 2020;39:101120. doi:10.1016/j.ctcp.2020.101120
38. Nacar MC, Nursal AF, Kuruca N, Yigit S. A circadian rhythm gene (PER3) VNTR variant as possible risk factor in cohort of Turkish females with primary dysmenorrhea. Nucleosides Nucleotides Nucleic Acids. 2022;41(9):900–909. doi:10.1080/15257770.2022.2085743




